Clinical Essentials of Chronic Lower Limb Ischemia- Lifestyle Limiting Ischemia- Vascular Surgery
- Selvaraj Balasubramani
- May 8
- 3 min read
Chronic Lower Limb Ischemia: Lifestyle-Limiting Claudication Study Guide
Definition and Overview
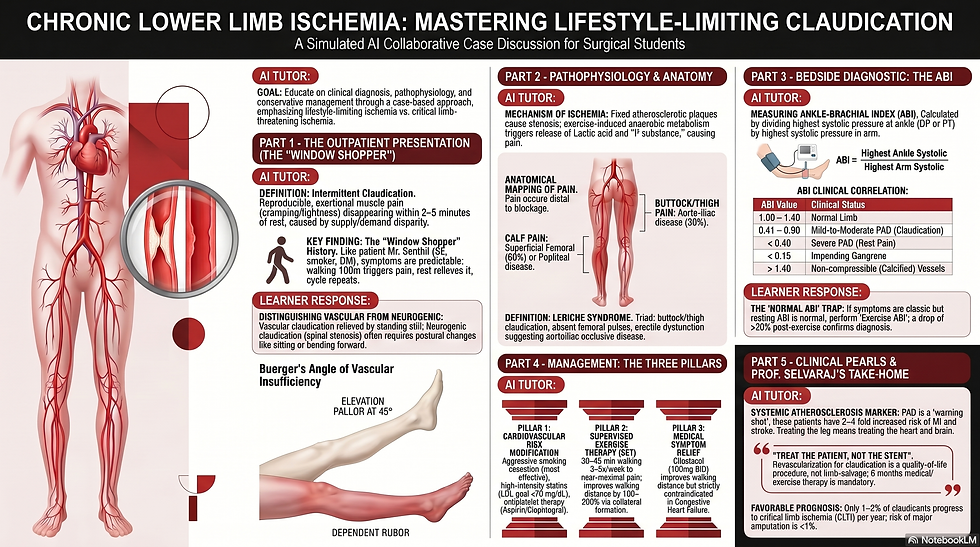
Lifestyle-limiting ischemia is a form of Peripheral Arterial Disease (PAD) in which atherosclerotic stenosis or occlusion reduces blood flow to the limbs.
It is primarily characterized by intermittent claudication—exertional pain that limits a patient's daily activities but does not pose an immediate threat of limb loss.
It is often described as a "warning shot," indicating systemic atherosclerosis and a significantly increased risk of myocardial infarction and stroke.
Pathophysiology
Fixed atherosclerotic plaques in the lower limb arteries (such as the superficial femoral or iliac arteries) restrict blood flow.
At rest, blood supply is sufficient; however, during exercise, muscle oxygen demand increases.
This creates a supply-demand disparity, leading to muscle ischemia and the accumulation of metabolic byproducts like lactic acid, which trigger pain.
The pain is relieved when the patient stops walking because metabolic demand drops to a level the stenotic artery can accommodate.
Clinical Presentation
The Classic History: Predictable and reproducible muscle pain (cramping, tightness, or aching) that occurs after walking a specific distance.
Relief Pattern: The pain is relieved completely within 2 to 5 minutes of standing still. It is not dependent on a change in posture (unlike neurogenic claudication).
Anatomic Correlations: The site of pain occurs distal to the arterial blockage:
Calf Pain: Suggests superficial femoral or popliteal artery disease.
Thigh/Hip Pain: Suggests iliac artery disease.
Buttock/Thigh Pain + Erectile Dysfunction: Known as Leriche Syndrome, suggesting aortoiliac occlusive disease.
Physical Examination Findings
Pulses: Pedal pulses (dorsalis pedis and posterior tibial) are often weak or absent. Bruits may be audible over the femoral arteries.
Trophic Changes: Chronic ischemia may cause shiny skin, loss of hair, thickened nails, and muscle wasting in the affected limb.
Buerger’s Test: A positive test shows pallor when the limb is elevated to 45 degrees and a "dependent rubor" (dusky redness) when the limb is lowered.
Diagnostic Pathway
Ankle-Brachial Index (ABI): The first-line bedside diagnostic tool.
Normal: 1.00 – 1.40.
Diagnostic of PAD: ≤ 0.90 (0.41–0.90 indicates mild-to-moderate disease).
False Elevations: Values > 1.40 suggest non-compressible, calcified vessels (common in diabetes or CKD), requiring a Toe-Brachial Index (TBI) for accuracy.
Exercise ABI: If symptoms are classic but the resting ABI is normal, the patient performs treadmill walking. A drop in ABI of >20% post-exercise confirms the diagnosis.
Duplex Ultrasound: The first-line imaging study to localize the level of stenosis and assess its hemodynamic significance.
CTA or MRA: Reserved for anatomic mapping only when revascularization is being planned.
The Three Pillars of Management
Pillar 1: Cardiovascular Risk Factor Modification
Aggressive smoking cessation (the most important modifiable factor).
High-intensity statin therapy (targeting LDL < 70 mg/dL).
Antiplatelet therapy (Aspirin or Clopidogrel) to reduce systemic cardiovascular events.
Strict control of blood pressure and diabetes.
Pillar 2: Supervised Exercise Therapy (SET)
The most effective non-invasive treatment for improving walking distance.
Involves walking to near-maximal pain, resting, and repeating for 30–45 minutes, 3–5 times per week for at least 12 weeks.
Pillar 3: Medical Symptom Relief
Cilostazol (100 mg BID) is a phosphodiesterase inhibitor that can improve walking distance by up to 50%.
Contraindication: It is strictly forbidden in patients with any history of Congestive Heart Failure (CHF).
Indications for Revascularization
In lifestyle-limiting ischemia, revascularization is a quality-of-life procedure, not a limb-salvage procedure.
It is reserved for patients with disabling symptoms that interfere with employment or basic daily living.
It should only be considered after a failure of medical and supervised exercise therapy (typically > 6 months).
Prognosis and Differential Diagnosis
Limb Prognosis: Very favorable; only 1% to 2% of claudicants progress to critical limb-threatening ischemia (CLTI) per year.
Systemic Prognosis: Poor if untreated; these patients have a 2 to 4-fold increased risk of death from heart attack or stroke.
Differential Diagnosis: Must be distinguished from Neurogenic Claudication (spinal stenosis), which is provoked by standing, relieved by sitting or leaning forward, and often associated with back pain.
For visual learners, please watch the AI-simulated case discussion video on Chronic Lower Limb Ischemia- Lifestyle Limiting Ischemia from my YouTube video embedded below.
Listen to my Apple Audio podcast on Chronic Lower Limb Ischemia- Lifestyle Limiting Ischemia with earphones for an immersive and transformational Learning Experience, especially for auditory learners.
Download the following Word document to learn 10 useful MCQs on Chronic Lower Limb Ischemia- Lifestyle Limiting Ischemia
Download the following Word document to learn 5 practical Clinical Pearls and 5 Pitfalls on Chronic Lower Limb Ischemia- Lifestyle Limiting Ischemia
Thank you for utilising my Learning Resources effectively. Kindly share your feedback to help me to improve my work further.

Comments