Lumbar & Spigelian Hernias- Abdominal Wall Swellings- AI Simulated Case Discussions
- Selvaraj Balasubramani
- 6 days ago
- 3 min read
Lumbar and Spigelian Hernia Study Guide
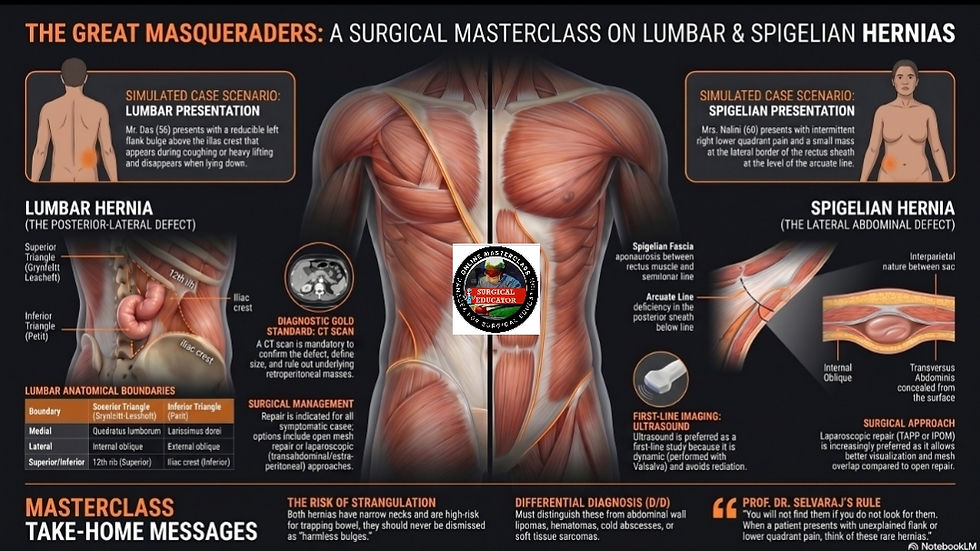
The Great Masqueraders
Lumbar and Spigelian hernias are known as the great masqueraders of the lateral abdominal wall because they hide deep within tissue layers, often cause chronic pain, and can strangulate without warning. A high index of suspicion and the use of imaging are critical for diagnosis.
Lumbar Hernia
Anatomical Boundaries Lumbar hernias are posterior-lateral defects that occur through two specific anatomical regions:
Superior Lumbar Triangle of Grynfeltt-Lesshaft: This is the most common site for herniation. It is bounded medially by the quadratus lumborum muscle, laterally by the internal oblique muscle, and superiorly by the 12th rib.
Inferior Lumbar Triangle of Petit: This region is bounded medially by the latissimus dorsi, laterally by the external oblique, and inferiorly by the iliac crest.
Clinical Presentation Patients often present with a history of flank pain. A bulge typically appears when the patient coughs or lifts heavy objects and reduces completely when they lie down.
Diagnostic Essentials: A CT scan is mandatory for any suspected lumbar hernia. It is used to confirm the diagnosis, define the exact size of the defect, and rule out underlying retroperitoneal masses that might be pushing the tissue outward.
Management
Surgical Indication: Elective repair is recommended for symptomatic hernias to prevent enlargement and incarceration.
Techniques: Small defects may be treated with primary closure and mesh reinforcement. Larger defects or those in obese patients often require open mesh repair with wide overlap or component separation.
Laparoscopic Approach: This is the modern standard for faster recovery and can be performed via transabdominal or totally extraperitoneal routes.
Spigelian Hernia
Anatomy and Pathophysiology A Spigelian hernia occurs through the Spigelian fascia, which is the aponeurosis located between the rectus abdominis muscle and the semilunar line. It most commonly occurs at the level of the arcuate line where the posterior rectus sheath is deficient.
The Interparietal Nature This hernia is interparietal, meaning the sac lies concealed between the internal oblique and transversus abdominis muscles. Because it sits deep to the external oblique aponeurosis, it is frequently not palpable as a discrete mass.
Clinical Presentation and Misdiagnosis Patients often report vague, intermittent pain in the lower quadrant. Because of its location and hidden nature, it is frequently misdiagnosed as appendicitis, diverticulitis, or abdominal wall hematomas.
Diagnosis Dynamic ultrasound is the preferred first-line imaging study. It allows the clinician to identify the fascial defect and hernia contents, such as omentum or bowel, while the patient performs a Valsalva maneuver.
Management
Surgical Indication: All Spigelian hernias should be repaired due to a high risk of strangulation caused by their typically narrow necks.
Laparoscopic Repair: Approaches such as TAPP or IPOM are increasingly preferred because they allow for full visualization of the defect and easy mesh placement with adequate overlap.
Open Repair: This approach is more challenging because the surgeon must divide the intact external oblique aponeurosis to access the concealed hernia sac before repairing the deeper muscular layers
Watch an AI-simulated case discussion video on Lumbar & Spigelian Hernias in the YouTube video embedded below for Visual learners.
Watch a video on discussions of 10 MCQs on Lumbar & Spigelian Hernias
Download the Word file below and learn 5 important Clinical Pearls & 5 Pitfalls on Lumbar & Spigelian Hernias
Listen to my Apple Audio podcast on Lumbar & Spigelian Hernias with earphones for an immersive and transformational Learning Experience, especially for auditory learners.
Thank you for utilising my Learning Resources effectively. Kindly share your feedback to help me improve my work further.
Comments