BURNS- Modern Management in Pediatric & Adult Population
- Selvaraj Balasubramani
- 3 days ago
- 3 min read
Updated: 3 days ago
Modern Management of Burns: Pediatric and Adult Study Guide
Definition and Pathophysiology
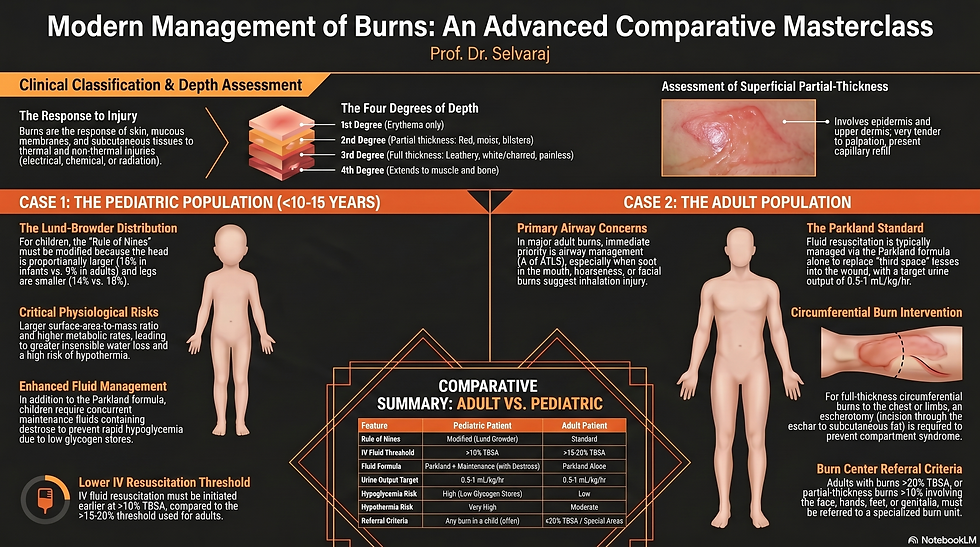
Burns represent the response of the skin, mucous membranes, and subcutaneous tissues to thermal, electrical, chemical, cold, or radiation injuries.
Heat causes coagulation necrosis of the tissue and the release of vasoactive peptides, leading to altered capillary permeability.
This permeability results in a significant loss of fluid, which can cause severe hypovolemia, decreased cardiac output, and renal failure.
The injury is categorized into three zones: the zone of coagulation (necrotic tissue), the zone of stasis (decreased perfusion that may recover or become necrotic), and the zone of hyperemia (viable tissue where healing begins).
Systemic changes following a major burn include respiratory bronchoconstriction, a threefold increase in basal metabolic rate, and a reduced immune response.
Pediatric Burn Management (Infants and Children)
TBSA Estimation: The standard Rule of Nines is inaccurate for children because their heads are proportionally larger and their legs are smaller.
For infants, the head and neck account for 18% of the Total Body Surface Area (TBSA), while each leg accounts for 14%.
Resuscitation Threshold: Intravenous fluid resuscitation must be initiated earlier in children than in adults, specifically when the burn exceeds 10% TBSA.
Fluid Formula: Children require a dual-track protocol using the Parkland formula (4 mL Ringer's Lactate x TBSA% x weight in kg) administered concurrently with weight-based maintenance fluids.
Maintenance fluids for children must contain dextrose to prevent rapid hypoglycemia due to their limited glycogen stores.
Physiological Risks: Children face a very high risk of hypothermia because their large surface-area-to-mass ratio accelerates heat loss.
Monitoring: The target urine output is 0.5 to 1 mL/kg/hr, and for small children, this may be monitored by weighing diapers if a Foley catheter is not used.
Adult Burn Management
Airway Priority: Airway management is the paramount priority in adult major burns, especially when inhalation injury is suspected.
Clinical signs of inhalation injury include facial burns, singed nasal hairs, soot in the mouth or sputum, hoarseness, and stridor.
Inhalation injury is the leading cause of death in burn patients within the first 48 hours due to upper airway edema and systemic poisoning from carbon monoxide or cyanide.
TBSA Estimation: The standard Rule of Nines is adequate for adults, where the head is 9%, each arm is 9%, each leg is 18%, and the anterior/posterior trunk are each 18%.
Resuscitation Threshold: IV fluid resuscitation is generally initiated for burns greater than 15% to 20% TBSA.
Fluid Formula: Adults are managed with the Parkland formula alone, giving half the total volume in the first 8 hours from the time of the burn; they do not require separate maintenance fluids.
Surgical Intervention: Circumferential full-thickness burns to the limbs or chest require an escharotomy—a surgical incision through the inelastic eschar to release pressure and prevent compartment syndrome.
General Management Principles and Referral
Initial First Aid: The burning process must be stopped, and the wound should be cooled with running water (2–15°C) for 20 minutes.
Burn Depth: First-degree burns involve only the epidermis (redness); second-degree (partial-thickness) burns are red, moist, and blistered; third-degree (full-thickness) burns are leathery, white or charred, and painless.
Wound Care: Small superficial burns can be treated with non-adherent dressings and twice-weekly inspections, while topical silver sulfadiazine is often used on deep burns to reduce infection risk.
Referral Criteria: Patients should be referred to a specialized burn center if they have partial-thickness burns over 10% TBSA, full-thickness burns over 5% TBSA, or any burns involving the face, hands, feet, genitalia, or major joints.
Other referral triggers include electrical or chemical burns, inhalation injury, circumferential burns, and burns in patients with significant comorbidities or associated major trauma.
For visual learners, please watch the AI-simulated case discussion video on BURNS- Modern Management in Pediatric & Adult Patients, from my YouTube video embedded below.
Listen to my Apple Audio podcast on BURNS- Modern Management in Pediatric & Adult Patients with earphones for an immersive and transformational Learning Experience, especially for auditory learners.
Download the following Word document to learn 10 useful MCQs + 5 Clinical Pearls + 5 Clinical Pitfalls
on Burns- Modern Management in Pediatric & Adult Patients
Thank you for utilising my Learning Resources effectively. Kindly share your feedback to help me to improve my work further.
Comments